By Philip Smallwood Cambridge University Press, 2023
A Review
This is a book of meticulous carefully researched scholarship. If like me, you are only dimly aware of literary criticism and still less of Samuel Johnson then you will learn a lot from reading this book though it will require some persistence. If you are familiar with the topics or indeed a literary scholar, then there is much detail to absorb and learn from.
Literary criticism is the comparison, analysis, interpretation, and/or evaluation of works of literature. It is essentially an opinion, supported by evidence, relating to theme, style, setting or historical or political context.
Samuel Johnson was an 18th century British scholar who made significant contributions to the fields of literature and writing as an author critic, essayist, and lexicographer. He was born in 1709 in Lichfield, England. In this book the author is clearly seeking to uncover the wisdom contained in his writing. Johnson was prolific, producing 208 essays for the Rambler every Tuesday and Thursday from1750 to 1752. He wrote 103 essays called the Idler and published in the newspaper The Universal Chronicle between 1758 and 1760. Johnson wrote a collection of biographies of the Lives of the Poets – a critical appraisals of 52 poets, most of whom lived during the eighteenth century. However, Johnson is probably best known for his Dictionary of the English Language published in 1755. It is regarded as one of the most influential dictionaries in the history of the English language. Johnson is admired for his witty definitions. For example, he wrote that oats are “a grain which in England is generally given to horses, but in Scotland supports the people”. He said that the true measure of a man is how he treats someone who can do him absolutely no good.
As a non-specialist in literary criticism, I see poetry as the ‘music’ of language. They both use language and sound to create meaning and evoke emotions. Both rely on rhythm, meter, and repetition to create a sense of structure and flow, and both can be used to tell stories, express emotions, and explore complex themes and ideas.
The author makes it clear that Johnson wrote from the criteria of the heart. Mathew Arnold wrote that Johnson’s utterances are valuable….because they come from a “great and original man”. The author might have added – “a man of great wisdom” – a quality that seems sadly lacking amongst current public opinion formers and requiring much clearer articulation for the modern context.
Johnson recognises the fragility of life. He writes that “Much of the pain and pleasure of mankind arises from the conjectures which everyone makes of the thoughts of others; we all enjoy praise which we do not hear and resent contempt which we do not see.” The “secret horror of the last is inseparable from a thinking being whose life is limited, and to whom death is dreadful. We always make a secret comparison between a part and the whole; the termination of any period of life reminds us that life itself has likewise its termination; when we have done anything for the last time, we involuntarily reflect that a part of the days allotted us is past, and that as more is past there is less remaining”.
The author skilfully weaves references to some of the great poets such as Pope, Drydon, Swift. Johnson wrote about the lives of numerous poets – as well as Shakespeare whose characters, Johnson recognised, speak “warm from the heart”, prior to thought or in its absence. Shakespeare is a poet of nature who permits access to nature beyond what reason affords in critical dialogue with its sometimes-cruel incomprehensibility. Johnson’s sense of the moral functioning of Shakespeare plays as a “system” goes far beyond their exploitation of propositional thought. Imlac (a character in Johnson’s novel, The history of Rasselas) observes that “Our minds like our bodies…are in continual flux …. but nature will find the means of reparation”. There is no man whose imagination does not sometimes predominate over his reason. The author points out that this work relates to the modern ideas of a “process philosophy” as developed by John Dewey, William James, Charles Sanders Pierce, and Alfred North Whitehead as it explores the unfolding of happiness, freedom, and the human condition.
The author reminds us that Johnson affirmed that “Poetry is the art of uniting pleasure with truth, by calling imagination to the help of reason”. Johnson commonly acknowledges limits to unhindered theoretical speculation….in the face of universal imponderables. The author makes two judgements – that Johnson prioritises what we feel over what we can imagine and that “the heart naturally loves truth”. Fanciful narratives that have no historical basis but nevertheless can retain their emotional force. Shakespeare’s The Tempest has a “sublime and amazing imagination…which soars above the bounds of nature without forsaking sense. The break between history and mythology may not always be as sharp as historians would like. The author speculates that we live in patterns, but we do not see them except from the distance that art affords us. Johnson wrote that the “great part of every writer is only the destruction of those who went before. The first care of the builder of a new system is to demolish the fabricks which are standing”.
In summary this is a book of great interest to all whether literary critics or not. It is a detailed source of literary cross references and contemporary analysis of the work of an influential thinker, Samuel Johnson.
A four-cause interpretation of Ray Dalio’s ‘Big Cycle’1
Almost all right-thinking decent people find the loss of life and damage to buildings and infrastructure in wars in Ukraine and the Middle East as entirely repulsive. Indeed, the violence is so severe that many are saying ‘enough is enough’. We have to learn to ‘rub along together’ – to have more tolerance and find peaceful coexistence even if we disagree about lifestyles, political governance and religious beliefs. We need a new peaceful world order.
Indeed, this the major message of my forthcoming book, ‘Climate Change is an Opportunity’2. We have an imperative, as never before, to change our ways. The entire human race is facing its greatest ever existential challenge, climate change. If we don’t change our attitudes towards each other the human race may face extinction. This is not an exaggeration.
Just as I had finalized the text of my book, I came across Ray Dalio’s book, ‘The Changing World Order 1. He sees what he calls ‘Big Cycles’ of world order which he traces from the 16th century dominance of the Dutch, the 19th century dominance of the British to the hegemony of the USA since 1945. He sees the USA today as in decline through debt burden, increased internal divisions and the rise of external disorder in its relations with China and others. He makes little mention of climate change but does recognize that’s acts of nature are important and climate change will be very costly in both money and quality of life.
World order is the framework of power and authority for diplomacy and world politics. It includes the norms, rules, institutions, and power dynamics that shape the behaviour of countries. For most of history, the structure of world politics has been multipolar. A number of great powers competed for influence and, collectively, determined the rules of the game. What sets the post-1945 Western order apart is that it was shaped overwhelmingly by a single superpower, the USA, underpinned by the United Nations, the World Trade Organization, the International Monetary Fund, and other international organizations that promote cooperation and collaboration among nations.
Dalio analyses the ‘Big Cycles’ from the 17th century Dutch through the 19th century British and the 20th century American. The Dutch set up a banking system with the guilder as Europe’s reserve currency that we would recognize today. A reserve currency is a foreign currency that is held in significant quantities by central banks or other monetary authorities as part of their foreign exchange reserves. Reserve currencies are used in international transactions, investments, and all aspects of the global economy. Britain after two world wars had huge debts and had to borrow from other countries. But the £ is still the fourth most-held currency after the $US, Euro, and Japanese Yen.
Dalio’s ‘Big Cycles’ comprise a rise, a top and a decline. They resemble Aristotle’s four causes as we shall see. Characteristics of nations on the rise include, strong leadership, education, inventiveness, culture, resource allocation and competitiveness. At the top of the cycle is strong income growth, markets, and financial centres. However, nations gradually become less productive, overextended, with a loss of competitiveness and growing wealth inequalities. Nations in decline have weak leadership, with massive debt, and internal conflict and even a form of civil war. The large debt is managed by printing money with a possible decrease in the value of the currency and inflation. Nations in decline may lose their reserve currency status if investors stop buying government debt or if they think the creditworthiness is decreased by unsustainable levels of debt, political instability, and inflation.
We can compare Dalio’s cycles to those of Aristotle’s four causes- formal, efficient, material, and final cause. Formal cause is the form of an object that give structure and shape. Efficient cause is the making of an object, material cause is what it is made of, and final cause is function – such as being a cell phone. However, a deeper modern interpretation3 is that a formal cause is a potential for becoming – such as the growth of an organism or the design of an artefact. An efficient cause is the bringing about of change, a material cause is an attainment of a state of affairs, and the final cause is an evaluation and anticipation of future states. The cycle is evolutionary, repeats and occurs at many different levels.
Nations on the rise in Dalio’s analysis are prospering through education, investment, and inventiveness. These are formal causes – prosperity is being designed and nurtured. Nations at the top of Dalio’s curve have efficient causes of change through strong growth, markets, and financial centres. The changes of culture and social norms are the very fabric of a society and hence a material cause. The economies attain the effect of gradually becoming less productive as people enjoy their successes. Decline begins when wealth inequalities grow resulting in internal conflicts, with large debts which are often countered by printing money. Leadership is weak and the decline ends with external conflict or revolution. Reserve currency status is lost. Examples are a) the ending of the Dutch Empire guilder as a reserve currency and b) the rise of the British Empire £ after Anglo-Dutch wars of the 17th and 18th century and c) the taking over by the US$ after WW 2.
In this four-cause analysis the decline is a final cause – but one that is anticipatory and evaluative. Thinking about the decline this way, leads us to a new kind of conclusion and new opportunities. As I have proposed in my forthcoming book a re-evaluation of the declining state suggests that rather than a possible conflict between the dominant nation and up-and-coming nation states such as the BRICS countries, we can and must develop a world vision of collaboration and co-operation that will tackle the consequences of climate change. BRICS include Brazil, Russia, India, China and South Africa together with new joiners Iran, Saudi Arabia, Egypt, Argentina, the UAE, and Ethiopia – all of whom have large populations, abundant resources, and growing economies. So, in summary, we could and should, reinterpret this stage of Dalio’s ‘Big Cycle’ not as a decline but rather as a final cause. We can anticipate a version of principled capitalism, as I have proposed, but interpreted by different nations in their own ways. The ten pillars of principled capitalism2 would stand to integrate and facilitate collaboration and co-operation. Strong leaders such as Ajay Banga President of the World Bank and Antony Guterres Secretary General of the UN are beginning to show us the way. In each country we should elect/choose political leaders who will take us into a new formal cause – a new potential for becoming a peaceful world order.
References
Dalio R (2021) The Changing World Order, Simon & Schuster, London
Blockley, D (2024) Climate Change is an Opportunity, CRC Press, USA
Blockley D, Smith G, Godfrey P, Kineman J (2022) Relational Holon Science and Popper’s 3 Worlds in engineering practice, Systems Research and Behavioural Science DOI: https://10.1002/sres.2906
We have an imperative, as never before, to change our ways. The entire human race is facing its greatest ever existential challenge. I wrote this new book because I feel a growing sense of looming disaster. Yes, we are making some progress through initiatives such as the ‘Green New Deal (GND)’ and the USA Inflation Reduction Act – so it’s not all gloom. The Intergovernmental Panel on Climate Change (IPCC) continues to provide important rigorous and balanced scientific information based on published literature. The UK and 77 other countries are committed to reaching ‘net zero’ greenhouse gas emissions by 2050.
The 2023 IPCC report states ‘There is sufficient global capital and liquidity to close global investment gaps……but there are barriers to redirect capital to climate action both within and outside the global financial sector.’ This latest announcement triggered the UN secretary Antonio Guterres to say ‘This report is a clarion call to massively fast-track climate efforts by every country and every sector and on every timeframe. Our world needs climate action on all fronts: everything, everywhere, all at once.’
Martin Wolfwrites ‘Pessimism about humanity’s ability to address climate change is understandable. Time is limited, talk plentiful and action negligible. But we can only start from agreement that there is indeed a threat worth addressing….. despair is not an option.’
We know what we need to do. The problem is doing it. How do we convince our politicians that more urgency is needed? Governments and industry are reacting too slowly. One of the key messages of my new book is that fear of national debt is holding us back.
Yeva Nersisyan and L Randall Wray, and separately Richard Murphy, are showing us how we can pay for the Green Deal. Nersisyan and argue that the Green New Deal is MEOW (Moral Equivalent of War). The basis of their argument is that affordability cannot be an issue for the sovereign USA government (or any sovereign state with fiat currency. They write ‘The costs of extinction of the human species—from the point of view of humans, at least—is beyond measure. Even if we calculate the costs of the GND as $93 trillion over the next decade, that is puny in comparison with the discounted cost of total destruction of human life on planet Earth.’
Murphy has proposed green quantitative easing to kick start economic activity to deliver a new green deal.
Modern Monetary Theory (MMT) exposes some myths around government deficits and debt. I wonder if you have ever heard of fiat money. Most non-economists haven’t. It is of central importance in understanding the economies of the UK, USA and others. Fiat means by decree. Fiat money is a currency that is declared legal tender by a government that has no intrinsic or fixed value and is not backed by any tangible asset such as gold. In other words, the currency only has value because the government says it does. The stability of the currency depends on the stability of the country’s economy. The country has monetary sovereignty in that it can spend, tax, and borrow its own currency without promising to convert it into gold or foreign currency at a fixed price. The government issues the currency whilst the rest of us use it. Understanding fiat money enables us to see that the economics of a country that issues fiat money is fundamentally different from the economics of a household or any other users of that currency. The government issues the money via the banks and recoups much of it back through taxation. It can never go broke. Indeed, government deficits create a surplus in the private economy. Inflation only occurs when supplies aren’t sufficient to meet demands. The theory of MMT is largely based on accounting practice and the flow of money. The British economist Wynne Godley pointed out orthodox economics has inconsistent stock and flows. MMT uses balance sheets to make sure the stock flows are consistent as I explain in the book. Nersisyan and Randall Wray write ‘……we can afford the real MEOW. We already have the financial wherewithal needed to afford whatever is technologically possible. We do not need to go hat-in-hand to rich folks to get them to pay for it. We do not have to beggar our grandkids to pay for it. We do not have to borrow from China to pay for it.’
In the book I call for us to do three things. First to recognize we become what we think, and that we need to think differently to change social norms. Second, we must learn to test what we are told more rigorously to tackle misinformation and social manipulation. Third, we must act to build trust. To do these things I propose a new form of capitalism called principled capitalism. It can emerge out of current liberal capitalism if we widen the ideas of utility as personal satisfaction and the profit motive to include all forms of obligations to each other and to nature. An obligation as a root reciprocal moral principle for any society of more than two autonomous rational beings. Values are the things we hold as important in the way we live. In short, the worth of what is the ‘good.’ Values determine our personal priorities such as education, wellbeing, honesty, truthfulness, loyalty, open-mindedness, consistency, and our corporate values such as sustainability, efficiency, creativity, ingenuity, and innovation. To act with good faith is to act reasonably. This implies that consent is not withheld by any of the parties unreasonably, depending on context. Under the law of tort, a duty of care is owed by each one of us towards any other to adhere to a reasonable standard of behaviour that will do no harm. It is an expression of the social contract by which we live and work together.
Obligations are a root reciprocal moral principle found in the ‘golden rule’ of all religions ‘do unto others as you would have them do unto you’ (Luke, Ch. 6, v 31).
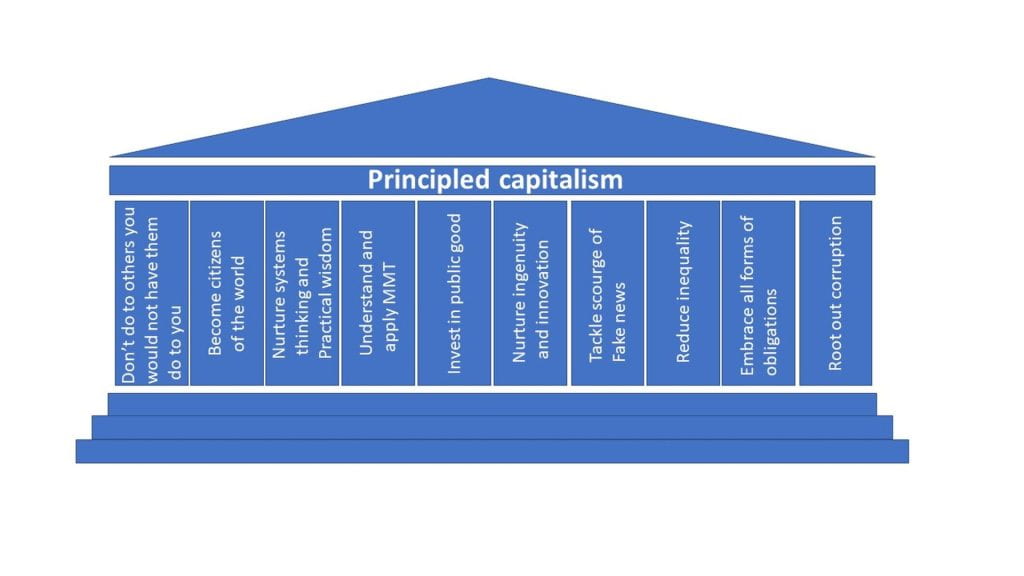
Climate change is a challenge and an opportunity – change we must if life on Earth is to survive as we know it. Meeting the challenge and taking to opportunities we can become citizens of the world defined by our interdependence and community. In my new book I suggest and discuss ten pillars of principled capitalism. Don’t do to others that you wouldn’t have them do to you, become citizens of the world, nurture systems thinking and practical wisdom, apply modern monetary theory, invest in the public good, nurture ingenuity and innovation, tackle fake news, reduce inequality, embrace all forms of obligation, and root out corruption.
I maintain that citizens of the world are ‘together people’ They recognize our interdependence and need for community. Being a world citizen is an active verb rather than a noun – a notion of doing something. Citizens look around, identify the domains they can influence, find collaborators, and engage with them. We must develop organizations to allow and encourage us to do so. The citizen story is a bigger story of who we are as human beings.
Why we need an international programme to develop systems thinking in the Citizen’s Story
A lot of uncertainty and not a little alarm has resulted from the UK September mini budget. It proposes cuts in income tax, reverses rises in National Insurance and Corporation tax, tightens benefit and trade union conditions, cuts stamp duty on properties, caps energy bills, scraps limits on banker’s bonuses, cancels VAT for overseas shoppers, and liberalises planning rules. It has yet to be approved by the UK Parliament.
The OBR (Office for Budget Responsibility) were not asked to cost out the plan and will not publish their deliberations until the end of October or November. The response of the markets was immediate. The £UK sank against the $US and then recovered. Interest rates rose and are rising. The IMF (International Monetary Fund) asked the UK Government to reconsider. The BoE (Bank of England) intervened to save pension funds from the effects of rising UK Bond prices and interest rates by temporarily stopping its Qualitative Tightening (QT – contracting the money supply) and buying Bonds (QE – expanding the money supply). A report from the United Nations Conference on Trade and Development (UNCTAD) released this week states that the alarm bells are ringing and a major course correction is needed—quickly—if the world is going to avert a painful economic slowdown and a global debt crisis. The world is headed towards a global recession and prolonged stagnation unless we quickly change the current policy course of monetary and fiscal tightening in advanced economies. The report calls on governments in advanced economies to avoid austerity and urges central banks to avoid trying to bring down prices by increasing interest rates.
We now have in the UK, a fiscal policy and a monetary policy pulling in opposite directions – yet both are inflationary. Reduced taxes increase demand by putting more money into people’s pockets, some of which they will spend and some of which they may save if they can, to offset it against future uncertainties. Raising interest rates increases the cost of mortgages. Quantitative Easing (QE) swaps illiquid government bonds for liquid cash to stimulate the economy – though the Bank of England says that is temporary. We must wait and see what the Bank of England decides about future interest rates and if it returns to Quantitative Tightening (QT).
All of this is happening at a time when unemployment is low.
Governments of the past have found it difficult to buck the financial markets when traders have lost confidence in their economic policy. Credibility is fragile, easily lost, and hard to regain. Problems in one financial market can spill over into others with unexpected and global consequences. Cuts to public spending can be damaging. Infrastructure is harder to repair as a way of stimulating longer term growth. The political damage is long lasting and weakens support for the parties and creates general disillusion with politics. It would be unfortunate if the phrase ‘Remember what happened in 2022’ became the new narrative. We do not want to reinforce the idea that financial markets ultimately get to say whether or when governments can expand their budgets. Nor do we want to hear that if investors decide that the government is behaving irresponsibly, they will refuse to supply the £ needed to pay for government spending. The UK government issues currency – it does not need to borrow from anyone.
So, the key question is what the UK government will do to improve the economy to increase supply and meet the growing demand. If it fails, then inflation will get worse.
Stephanie Kelton emphasises in her book ‘The Deficit Myth’ that countries with a fiat currency cannot go bankrupt. The reason is simple – they issue currency whilst the rest of us use it. Fiat just means ‘by decree’. The £UK is a fiat currency as is the $US and the Japanese Yen ¥. It is a common mistake, she says, to equate household budgeting with that of a country with a fiat currency. Individuals, households, and companies are currency users so if their income does not match their expenditure, they will eventually be bankrupt. The UK government is not so constrained as it is a currency issuer. Indeed, the government has a year-on-year deficit as its spending exceeds its income. Its income is chiefly taxes. That spending goes into the economy as a surplus. The accumulated deficit over time is the national debt (which really isn’t – we need a new word for it). But we have to be cautious, the UK government cannot simply put money into the economy willy-nilly – there is one big constraint, inflation. If there aren’t enough supply resources to meet demand, then inflation becomes a problem. Current inflation was triggered by energy imports paid for in $US but has now become embedded right across the economy.
The UK problem now is therefore one of insufficient supply to meet demand. It is not helped by unemployment being so low after Brexit and Covid-19 because one of the ways to strengthen supply is to recruit more labour. Other ways commonly quoted as helping to increase supply are, investment in the public sector, education, and training, better working conditions whether in the workplace or through better housing and health, reducing regulations, free trade agreements and reduced welfare to increase incentives for people to get a job.
But there is one further way of improving supply that is hardly ever mentioned yet could potentially be very powerful. It is to move emphasis beyond formal education and training to one of helping and encouraging people to ‘learn how to learn’. We are living in a new age of uncertainty and complexity with constant flux. The ever-increasing pace of change is demanding on all of us and many people flounder – some so seriously that they refuse to engage with IT altogether. But herein is an opportunity. Companies and individuals that learn how to learn faster than their competitors get a considerable competitive advantage. Inbuilt in that process lies a systems thinking approach to life. Systems thinking can be hard to grasp at first. In simple terms it is ‘joined-up’ thinking but it is more than that. It is an approach to understanding the world and making decisions individually and collaboratively in teams. Systems thinkers look for interconnections – they are social joiners. Out of it emerges a different approach to the processes of solving problems. Rather than isolating and fixing a problem they see the wider context and the ways in which all of the parts to the system interact. These ideas lead to new concepts such as seeing the natural and social world in layers or levels, of parts and wholes and how characteristics in those levels emerge from interactions between parts at lower levels. Another way of understanding is to see systems thinking as about getting the right information (what) to the right people (who) in the right way (how) in the right form (where) at the right time (when) for the right reason (why). If adopted by individuals, organisations, companies, and government then widespread use of systems thinking could improve efficiencies as well as providing better working conditions, more innovation and self-satisfaction – in short human flourishing.
Collectively we must try to persuade governments around the world to invest, at this time of financial crisis, in this novel form of raising productivity. We want to see the wholesale adoption of systems thinking to learn how to learn how to adapt, innovate and become ingenious in the sense that it is the root of the word engineer. It nurtures practical wisdom – being inventive, resourceful and skilful through direct practical experience. Such moves would be a natural partner to attempts to move away from the consumer story of economics to the Citizen’s story of economics as promoted by Jon Alexander and others.
Why the financial crisis after the Mini-Budget needs some systems thinking
As Kwasi Kwarteng reverses his decision to abolish the 45p rate of income tax for anyone earning over £150k after only two weeks, the markets are perhaps understandably volatile. Where will this lead? How is the average non-economist to understand the situation?
UK bonds surged after the Bank of England said it would carry out temporary purchases of long-dated UK bonds and delay planned sales of debt. The response seemed at first sight to be a reversal of their current QT (Qualitative Tightening) monetary policy back to QE (Qualitative Easing) and simply a shifting of the deck chairs since the BoE is wholly owned by the UK Government.
Deeper examination exposes a much more complex system that requires better thinking about system behaviour.
In various articles, MMT economist Stephanie Kelton, historian Adam Tooze and former multi-asset fund manager Toby Nangle, have explained how overly complex financial instruments have created the chaos. The inevitable unintended consequences have exposed an unsuspected and dangerous trigger mechanism in the UK financial system – that of rapidly rising interest rates.
Hedging is a strategy designed to limit risks in financial assets. Last week pension funds that hold hedging bets against the possibility that interest rates will fall – so-called liability-driven investment strategies (LDI) – were called suddenly to find more capital. Pension funds have been holding around £1.5 trillion of assets which they hedged to match pension funds’ liabilities (future payments to pensioners).
According to Toby, the Pensions Regulator estimates that every 0.1 percentage point fall in UK gilt yields increases pension fund liabilities by £23.7bn. In the decade to December 2020, long-dated, 25-year gilt yields fell by more than 3.5 percentage points and so scheme liabilities increased by £960bn (about 40 per cent of GDP). Pension schemes can’t control wild swings in their liabilities. But using LDI they can invest their assets to reduce the effects. The funds hedge volatility by moving assets into bonds. Unfortunately, few pension schemes have the funds to do this. So instead, they invest a portion of their assets in liability-matching bonds and a portion in corporate credit, equities, and property. They then hedge the risks of that strategy with derivatives, with bonds as collateral. Derivatives are complex contracts that derive value from an underlying asset. The depend on price fluctuations of the asset in various ways depending on the contract. The pension funds hope that growth will deliver decent returns and make them fully funded while the derivatives will desensitize them to future interest rate swings. Historically the results have been good. However, pension funds became vulnerable to enormous quantities of leverage – the use of borrowed money.
That risk was starkly exposed when the trigger was pulled, and interest rates shot up. UK pension funds also invest in foreign bonds so as the pound sterling dropped, they faced margin calls on foreign exchange derivatives. A margin call occurs when a broker requires that you make a deposit into your investment account because your margin position—the amount you owe the brokerage firm—has become too large. Some commentators have seen similar vulnerabilities in the US market.
Why does this all show the need for systems thinking? The first and obvious reason is the need to be aware of and specifically look for unintended consequences within complex systems. It is difficult for any one individual to spot all that might emerge and ‘slap you in the face’ but that leads to the second reason -to expect and look for possible interdependencies. The third reason is the need for team working and good leadership. Teams can also suffer from groupthink – so the broader the mix of skills in the team and the more they are encouraged to question through critical discussion, the more they are like to spot potential problems. A tenet of systems thinking is that whilst it is sensible to mitigate risks, they can never be removed all together. So, a very close watching brief of unfolding processes is needed – especially when so much money is at stake. As the sociologist Barry Turner recognized in the 1960s situations like the one described do not just happen – they incubate or emerge from unknown or unexpected interdependencies.
The action by the BoE is akin to a superb cricketing catch at first slip. Financial systems are fortunate to have such a back stop – the BoE as a lender of last resort. People should note that had this been a physical engineering or medical system there would be no back stop to rescue the situation and lives as well as money would possibly be lost. I would suggest that those who design complex financial packages need to be more aware of, and actively look for, the unintended consequences of what they plan and the potential for harm to others.
The Structure of Health and Social Care Services UK
A ‘Thought Piece’ – for discussion
by Gordon Stirrat1, David Blockley2, Kirsty Alexander3 & Sabrina Phillips4
1 Emeritus Professor of Obstetrics & Gynaecology, University of Bristol, UK.
2 Emeritus Professor of Civil Engineering, University of Bristol.
3 GP & Chair Bristol North and West Locality Leadership Group at Bristol, North Somerset and South Gloucestershire CCG, UK.
4Alliance Director (Interim)| Lambeth Living Well Network Alliance
Introduction
The United Kingdom’s National Health Service (NHS) was launched on 5 July 1948 with three underlying principles – the services were for everyone; healthcare was free; and provision of care was based on need rather than the ability to pay. In the intervening 72 years it has developed into an extremely complex organisation and one of the world’s largest employers. Because of its cost to the national exchequer, its organisation and funding have inevitably become matters of great political significance and debate. The general population has developed a great emotional attachment to ‘the NHS’ vividly expressed in, for example, Danny Boyle’s 2012 Olympic ceremony when, at one point, the floor of the stadium was occupied by a host of angelic nurses and 300 NHS beds filled with bouncing children. On the 60th anniversary of the foundation of the NHS Michael Rosen wrote his poem, ‘These are the Hands’, in praise of the mundane but vital contributions of healthcare workers. It has come back to prominence during our current tragic Covid-19 pandemic made even more poignant by the fact that Michael himself has been very seriously ill due to the virus. He has, thankfully survived and is gradually feeling better. Also, during the pandemic many of us have, along with our neighbours, gone out to clap on Thursday evenings as a sign of our support for ‘the NHS’ and the frontline workers coping with pandemic.
To many people in the UK, those working in GP surgeries and hospitals that deliver health (but not social) care are ‘the NHS’. The reality is far more complex, and we suggest that the structure of Health and Social Care Services UK, including the NHS and social care, and how the system reports and is accountable to Government and the public are all unnecessarily complex and opaque.
A complex structure
The Department of Health and Social Care (DHSC) is the Government body responsible for implementing policy in England. It delegates the work to NHS England. It is accountable to the Cabinet, Parliament, and ultimately to the general public. Health policy and implementation is devolved to the Scottish and Welsh governments and the Northern Ireland assembly. England is the only one of the 4 UK administrations to have a quasi-market but all use performance targets.
The NHS is complex set of organizations which, for the most part, work quite well despite a myriad of sub systems. A number of authors have referred to this complexity (1, 2, 3, 4) and, for example Powell (4) says ‘The leadership of the NHS seems fractured……a system under siege where success isn’t celebrated but failure is catastrophised’ We need ‘to build the confidence of the people who hold the problem.’ Attempts to explain the complex systems are necessarily partial (5, 6, 7). Good people can make a poor system work well but when pressures overwhelm them failure can be catastrophic (8). The NHS England long term plan (9) recognises the issues and states that the NHS will move to a new service model with ‘properly joined-up care…..creating genuinely integrated teams….with Integrated Care Systems (ICSs) everywhere by April 2021. ICSs will ‘deliver the ‘triple integration’ of primary and specialist care, physical and mental health services, and health with social care………Breaking down traditional barriers between care institutions, teams and funding streams.’ The intention of the plan is that providers, commissioners, local authorities and others will together locally plan and integrate care to meet the needs of their population. This initiative has grown out of sustainability and transformation partnerships and is the latest in a long line of NHS organisational changes. Currently there are 18 ICSs but demonstrations of progress are sparse (10).
How will integration be successful?
What are the incentives that will make integration work? Why should the many providers take responsibility for the total care of the whole population for probably less resource – when they have very little control over all the parts?
Everyone in the NHS shares a strong common purpose of ‘caring for our patients’. But does that translate into more detailed shared purposes at the various levels of the sub-systems?
We suggest that the key to driving change should be ‘influencing from the bottom up’ and not more ineffective ‘top-down’ centralisation (11). When policy decisions for change make sense to those ‘at the coal face’ they will respond. However, that response is conditional on the need for change to evolve up and down through the entire system. Policy makers and those allocating resources should alter, and integrate, some of the factors that will incentivise the ‘coal face’ individuals and organisations to work differently. A particularly important aspect of that incentivisation is that adequate resource follows activity without waste through unforeseen issues. For example, hospitals may initiate medication for a patient for which they have a particular financial deal, but the primary carers are not part of the deal and the medication may become very expensive for them.
The various parties to Integrated Care must also be aware that their potential partners may be fearful of extra work and responsibility being ‘dumped’ onto them. Sometimes, for example, individual GPs may be reluctant to hold challenging risks that hospital staff, with their more collective responsibility, may not be exposed to. If a patient dies during hospital treatment after a late diagnosis of bowel cancer caused at least partly through unintended delays (in the systems and perhaps also by the behaviour of the patient) the GP may find himself/herself in the spot light of blame by relatives, for not diagnosing quickly enough.
Making integrated care work has been variously described as ‘pushing a boulder uphill’ or ‘swimming against the tide. For example, differing financial incentives may produce perverse consequences. The commissioner/provider split and ‘payment by results’ (where income is proportional to activity) sometimes leads to a tick-box culture when used for some parts of the system. Block contracts for others do not incentivise improvements. Payment models have to encourage closer working around the needs of patients by sharing ‘pain and gain’ in an agreed manner. Co-operating organisations in the public and private sectors may have different bureaucratic constraints and work to different priorities and time scales as they attempt to adjust with agility to rapid changes. Organisational culture (in simple terms, the way that things are done – including the unwritten rules that influence behaviour and attitudes) can often dominate strategic aims. Some of the factors that influence culture include: leadership, deployment of resources, clarity of structure and processes, values and traditions. Success rests on leadership that overcomes professional silos and tribalism with good IT and access to targeted data – to harmonise strategy and culture.
There is little evidence of an equivalent attention to the ‘joining-up’ the proliferation of higher level non-local fragmented organisations reporting to or sponsored by the DHSC. The drive for integration ‘at the coal face’ does not appear to be reflected at the top of the NHS. There seems to be no unifying concept around which the integration can coalesce nationally. Without that there is a significant risk of regional ad hoc solutions that may not join-up across geographical/national boundaries.
Understanding the complexity through ‘systemic processes’
We suggest that the entirety of the health and social care system may be better understood by identifying its existing ‘systemic processes’. In saying this we do not imply the need for yet another total re-organisation. Rather we are suggesting an approach that could help the NHS system evolve into a more ‘joined-up’, less fractured and more integrated ‘whole’ across regional boundaries.
First, we need to describe the concept of a ‘systemic process’. This is not a sequence of events as in a flow chart (11). Neither it is simply a series of actions towards an end. Rather it is a reconceptualization of process as a potential that drives a flow of change – just as the volts of a battery drive an electrical current or water pressure drives the flow of water. A systemic process captures what people actually do and how change happens. In human systems the potential is contained in answers to questions ‘why’ – purpose, aims and objectives. The change is contained in answers to questions ‘who, what, where, when’. The transformation of the flow from one ‘state of affairs’ to another is contained in answers to questions ‘how’. The aim is to capture a systemic process as delivering the right information ‘what’ (data as performance indicators, success criteria and shared care records), for the right reasons ‘why’ (purpose), to the right person or organisation ‘who’ (role, stakeholder), in the right way ‘where’ (context) and at the right time ‘when’. Systemic processes are wholes and parts at the same time. They are ‘being things’ that change through natural forces – living or inanimate. You and I are ‘being’ wholes as individuals and yet also parts of family and social groups. As individuals ‘wholes’ we are made of parts such as our muscular skeleton structure and digestive systems. We are as we are because the parts collaborate to form the whole – in other words we show ‘emergent’ characteristics (12).
Applying these ideas to the structure of organisations we see logically related layers of interacting and interdependent systemic processes. For the totality of health and social care services this should encompass all of the organisations in and related to the NHS, including local authority social care and private companies. The successful delivery of a systemic process emerges from the success of sets of processes in the next layer down. An important part of the identification of these lower processes is that their successes are jointly necessary and sufficient for the process above – there is an explicit logical relationship connecting defined success, in all of its manifestations, at every level. It is also important to note that the layers are not hierarchical power structures. Rather they are levels of abstraction from setting policy down to detailed implementation. The attributes of each and every systemic process can be grouped under the headings of why, how, who, what, where and when. At each level the attributes can be identified by multiple players in a common format and implemented on a secure intranet to be accessed by those given authority to do so. Each and every process should have one ‘process owner’ responsible for leading the players involved in that process in detecting and monitoring progress, identifying unintended consequences and agreeing the required actions to steer the process to success (i.e. meeting purpose/aims/objectives) and avoiding failure.
We see the NHS as an ecology of interdependent relations and interactions between systemic processes. Survival and continued success depend on being able to generate an internal ecology of adaptive decision-making at all levels. It may be helpful to imagine each systemic process as a jigsaw piece. The ‘process pieces’ are connected to other pieces not by their interlocking shape but by recording their ‘neighbouring’ connectivity as an attribute and by enacting that connectivity by sharing relevantauthorised messages (composed by attributes why, how, who, what, where when). Creating the ecology may then be achieved by identifying, at a particular level, neighbouring processes and building them into clusters – just as you might piece together areas of a jigsaw. Practically it is helpful to name each piece of the jigsaw, each systemic process, using the present participle or ‘ing’ form such as ‘Doing something’ – ‘Testing a blood sample’ or ‘Diagnosing a condition’. An advantage of the approach is that the essence of what people actually do and how change happens is being captured. Then by growing and connecting clusters of systemic processes eventually a ‘whole system’ of layered clusters emerges. What is more during this ‘piecing together’ or ‘cluster building process’ changes and improvements will suggest themselves. For example, points of strategic dissonance may become apparent. This happens when an organisation hangs on to the old ways of doing things for too long because of a disconnect between actions and intent or purpose at any given level. For more on the details of this approach see (13, 14)
The organisations reporting to the DHSC seem to be contributing to seven high level systemic processes as shown in Table 1. There are, of course, many more organisations that cannot be included in the table.
Table 1: The 7 High Level Systemic Processes of Health and Social Care Services UK
Process
Examples
Role/Comment
Commissioning care
NHS England, Scotland, Wales and Northern Ireland
Commissions NHS services and is accountable to Ministers of Health
Clinical Commissioning Groups (CCGs)
Groups of GPs who purchase acute care on behalf of patients Accountable to NHS England.
Public Health England, Scotland, Wales & N Ireland
Arms-length Non-Departmental Public Bodies commissioning services to improve health & address inequalities Accountable to Ministers
Providing care
General Practitioners
Provision of primary care to patients under contract to Dept of Health & Social Care (DHSC)
NHS Trusts
Acute Hospitals in England & Wales
NHS Foundation Trusts
serving either a geographical area or a specialised function. (Do not yet have Foundation Trust status)
Supplying (including Special Health Authorities)
NHS Business Services Authority
Supplies business services
NHS Blood and Transplant
Supplies Blood and transplant organs.
NHS Digital
Supplies informatics
NHS Resolution
Deals with legal claims
NHS Counter Fraud Authority
Special health authority fighting against fraud, bribery and corruption in the NHS.
Regulating
Care Quality Commission
Regulator for health and social care
Human Fertilisation and Embryology Authority
Regulator of fertility treatment
Human Tissue Authority
Regulator of use of human tissue
+ 3 others
Medicines and Healthcare Products Regulatory Agency, Administration of Radioactive Substances Advisory Committee & National Data Guardian
Advising
National Institute for Health and Care Excellence
Purpose is to advise NHS on what constitutes good quality care.
Chief Medical Officers
Reports to and advises Secretary State for DHSC plus other Government Departments
Chief Scientific Officers
Employed by NHS England and leads healthcare science, advises all Government Departments & Chairs SAGE
Cabinet Office Briefing Rooms
Advises Cabinet on crisis and emergencies Accountable to Cabinet
Commission on Human Medicines
Advises on safety & use of medical products
+ 18 others not identified here
Educating
Health Education England, Scotland, Wales & N Ireland
Purpose is to support education and training An Arms-Length NDPB (Non-Departmental Public Body) Accountable to DHSC
Social Care Institute for Excellence
Independent agency that provides knowledge, evidence and accredited training for social care Accountable to Sponsors?
Researching
National Institute for Health Research
Receives funds for research. Accountable to DHSC.
The success of each of these seven systemic processes depends on (and logically related to) the successes of many lower layers of systemic processes. For example, NHS England allocates budgets to Care Commissioning Groups (CCGs), and so a necessary but not sufficient condition for successful financial outcomes for NHS England depends on successful outcomes for the CCGs. Social care is shared between DHSC and the Ministry of Housing, Communities & Local Government. Advising is delegated to many disparate sources with the consequent risk of inconsistency. Educating is delegated to Health Education England and the Social Care Institute for Excellence which in turn relies on the Royal Colleges and Universities. Research is delegated to the National Institute for Health Research and the Medical Research Council and onto the Universities and research centres. Clearly identifying all systemic sub-processes in the system is a considerable task. But it is a task that can and must be spread across all the players/actors involved in each and every process and captured on a national intranet.
We suggest that by structuring our thinking around these systemic interacting and interdependent processes we could achieve six objectives:
Provide a simple overview of the whole organisational structure that everyone can understand and appreciate which can be traced right down to the detailed ‘caring for patient’ processes.
Allow people to identify overlaps and interdependencies. For example, the 23 advisory organisations could possibly be streamlined to co-ordinate advice and avoid incongruity and inconsistency. Could the 8 regulating organisations be consolidated to avoid conflicting data and performance requirements?
Enable caring for the sick, caring for public health and the vulnerable be under one ‘umbrella’ to avoid inconsistencies of policy over the longer time scales than politicians are typically in post.
Enable a common data structure for the why, how, who, what, where and when attributes of each systemic process – important to avoid different groups using different data structures that cannot easily be shared and for data exchange via an intranet, with appropriate permissions to sensitive data, and the monitoring of progress and interventions to steer processes towards success.
Enable all those involved in delivering success for the NHS to identify how the necessary and sufficient conditions for the success of systemic processes at the ‘coal face’ feedback into success and deficiencies at higher policy levels
Permit us to clarify
pathways of precise terms of delegation and accountability – in particular;
how decision makers at all layers of the system delegate responsibilities down through the layers of processes – for example from government to NHS England and others to workers at the ‘coal face’ and ultimately to the patients;
how decision makers at all layers of the system are accountable up through the layers – for example from hospital ward care to Trust Boards, CCGs, NHS England and to government, parliament and ultimately to the public;
remove, reduce or ameliorate inconsistencies between policy and practice;
improve adaptability of response to unintended consequences and future unknowns such as pandemics and potential impacts from climate change.
Conclusion
The structure of Health and Social Care Services UK reporting to Government seems unhelpfully complex and opaque. We suggest a rationalisation using a ‘systems thinking bottom-up’ approach would be more likely to succeed than yet another top down reorganisation.
Rethinking the interactions between existing organisations around ‘systemic processes’ could arguably bring considerable benefits including cost savings, better co-ordination, less ‘admin’ stress on staff at the ‘coal face’ and provide more organisational adaptability in an uncertain future.
Ultimately ‘systemic processes’ could help everyone deliver better patient care because that is the impelling purpose of the NHS.
References
Timmins, N (2018) The World’s Biggest Quango: The first Five Years of NHS England, The King’s Fund & The Institute for Government, UK
Hudson, A (2016) Simpler, Clearer, more Stable: Integrated accountability for integrated care, The Health Foundation, UK
Integrating Health and Social Care Services in NHS England
by Stirrat, GM1, Blockley D I2, Alexander K3, Phillips S4
1 Emeritus Professor of Obstetrics & Gynaecology, University of Bristol, UK.
2 Emeritus Professor of Civil Engineering, University of Bristol.
3 GP & Chair Bristol North and West Locality Leadership Group at Bristol, North Somerset and South Gloucestershire CCG, UK.
4 Alliance Director (Interim)| Lambeth Living Well Network Alliance
Summary
A recent UK Government draft Heath White Paper follows the NHS England long term plan when it states that NHS England requires “a new framework that builds on changes already being made as well as building in the flexibility to support the system to tackle challenges of the future”. At present the structure of Health and Social Care Services UK reporting to Government seems unhelpfully complex and opaque. The purpose of this paper is to contribute to the building of a new framework by developing our previous suggestions that identifying and using ‘systemic processes’ can help facilitate the integration of England’s Health and Social Care services. We highlight some of the critical issues that are currently hindering integration and set out a new way of understanding the structure of NHS England through an ‘inside-out’ analysis of systemic processes. We describe and give three examples of existing systemic processes as ‘Consulting a patient’, ‘Enhancing a Single point of access’ -to mental health services and ‘Delivering health and social care services England’. Rethinking the interactions between existing organisations could arguably bring considerable benefits including cost savings, better co-ordination, less ‘admin’ stress on staff at the ‘coal face’ and provide more organisational adaptability in an uncertain future. Ultimately our suggestions are aimed at helping people to deliver better patient care – the impelling purpose of the NHS.
Purpose
The purpose of this paper is to develop our suggestions made previously [4] that identifying and using ‘systemic processes’ can significantly facilitate the integration of NHS England Health and Social Care services. Specifically, our objectives are to:
highlight some of the critical issues that are currently hindering integration,
set out a new way of understanding the structure of NHS England and the way it works through an ‘inside-out’ analysis of systemic processes,
describe and give examples of some NHS systemic processes,
outline a strategy for identifying and improving them across the entire health and care community,
reflect on the possible improved outcomes.
Issues that hinder integration
In a previous report [4] we have highlighted that the NHS is complex set of organizations which, for the most part, work quite well despite a myriad of sub systems. We noted that other authors have also referred to this complexity [5, 6, 7, 8] and, for example Powell [7] says “The leadership of the NHS seems fractured……a system under siege where success isn’t celebrated but failure is catastrophised”. We need “to build the confidence of the people who hold the problem.” Attempts to explain the complex systems are necessarily partial [9, 10, 11]. Good people can make a poor system work well but when pressures overwhelm them failure can be catastrophic [12].
In [4] we asked what are the incentives that will make integration work? Why should the many providers take responsibility for the total care of the whole population for probably less resource – when they have very little control over all the parts?
The pandemic has demonstrated to all that everyone in the NHS shares a strong common purpose of ‘caring for our patients’. But does that translate into more detailed shared purposes at the various levels of the sub-systems? We see at least 6 groups of issues that currently hinder integration.
Resources – where adequate resources do not follow activity without waste through unforeseen issues. For example, the cost of drugs from commercial pharmacies (and thus to the NHS overall) is considerably greater than the same drugs from hospital pharmacies Hospitals may initiate medication for a patient for which they have a particular financial deal, but the primary carers are not part of the deal and the medication may become very expensive for them. When payment models do not encourage closer working around the needs of patients by sharing ‘pain and gain’ in an agreed manner then integration will be harder to achieve.
Organisations – the various parties to Integrated Care have to be aware that their potential partners may be fearful of extra work and responsibility being ‘dumped’ onto them. Sometimes, for example, individual GPs may be reluctant to hold challenging risks that hospital staff, with their more collective responsibility, may not be exposed to. If a patient dies during hospital treatment after a late diagnosis of bowel cancer caused at least partly through unintended delays (in the systems and perhaps also by the behaviour of the patient) the GP may find himself/herself in the spotlight of blame by relatives, for not diagnosing quickly enough. Co-operating organisations in the public and private sectors may have different bureaucratic constraints and work to different priorities and time scales as they attempt to adjust with agility to rapid changes. Organisational culture (in simple terms, the way that things are done – including the unwritten rules that influence behaviour and attitudes) can often dominate strategic aims. Some of the factors that influence culture include leadership, deployment of resources, clarity of structure and processes, values and traditions. Success rests on leadership that overcomes professional silos and tribalism with good IT and access to targeted data – to harmonise strategy and culture.
Targets that are set top down without adequate consultation can lead to perverse behaviour. For example, waiting list targets resulted in requests for investigations and letters of referral being hidden from the doctors so that the patient was not put on an already “over target” waiting list. During the pandemic urgent cases were delayed because some doctors were not permitted to see the requests. Doctors and other staff were being told to use particular “pathways” and follow “guidelines”. Because the hospitals will not defend the staff if they stray from the guidelines then they effectively become directives. This leads to ossification of thought and procedure.
Leadership – top-down control of the NHS is seen by many to be inefficient and has hindered much of its work – particularly during the pandemic. Nevertheless, it can be effective when the main task is relatively simple, for example immunisation (once all the vaccine is available). However, diagnosis and treatment processes for individual patients are not simple – they are beyond the abilities of top-down management to control. Leadership cannot come from managers who do not understand or who are not qualified to do the job. The old system of consultant firms in the hospitals worked because the person in charge knew what they were doing. Likewise, the sisters on the wards and the matron in the hospital were a good combination of knowledge and experience. During the pandemic doctors in the NHS were told not to use various drugs that they might have wished to repurpose – such as ivermectin, hydroxychloroquine and dexamethasone. Until double blind trials had been undertaken these drugs were forbidden from use. This was seen by many as an unhelpful interruption of clinical freedom with consequent harm to patients.
Feedback and Learning – a consequence of top-down control is that staff are not encouraged to put their ideas forward. Some live-in-fear of their jobs if they blow thewhistle to anybody other than their line manager – the very person that they often wish to report. Organisational learning requires more freedom of expression.
Integrating at all levels – there is little evidence of an equivalent attention to ‘joining-up’ the proliferation of higher level non-local and fragmented organisations reporting to or sponsored by the DHSC. The drive for integration ‘at the coal face’ does not appear to be reflected at the top of the NHS. There seems to be no unifying concept around which the integration can coalesce nationally. Without that there is a significant risk of regional ad hoc solutions that may not join-up across geographical/national boundaries.
Systemic Processes
In [4] we suggested that the entirety of the health and social care system may be better understood by identifying its existing ‘systemic processes’. The purpose would be to evolve a more ‘joined-up’, less fractured and more integrated ‘whole’ across regional boundaries.
A systemic process [17] is not a sequence of events as in a flow chart [14]. Neither it is simply a series of actions towards an end. Rather it is a reconceptualization of process as a potential that drives a flow of change – just as the volts of a battery drive an electrical current or water pressure drives the flow of water. A systemic process captures why and what people actually do and how change happens.
The primary innovative characteristic of systemic processes is that they are structurally self-similar – just like the pieces of a jigsaw. Process ‘pieces’ form clusters and clusters of clusters which we can think of as layers of parts of the whole. The processes are, of course unlike a jigsaw, dynamic and ever changing. Systemic ‘jigsaw’ processes capture that change. Change derives from a potential that drives a flow (or dually from flow that creates potential). In classical physical systems potential is electromagnetic or gravitational and flow is movement. For example, voltage, current and velocity, force. In human affairs the potential is contained in answers to questions ‘why’ – purpose, aims and objectives. The change is contained in answers to questions ‘who, what, where, when’. The transformation of the flow from one ‘state of affairs’ to another is contained in answers to questions ‘how’. The aim is to model the right information ‘what’ (data as performance indicators, success criteria and shared care records), for the right reasons ‘why’ (purpose), to the right person or organisation ‘who’ (role, stakeholder), in the right way ‘where’ (context) and at the right time ‘when’.
Systemic processes are wholes and parts at the same time. They are ‘being things’ that change through natural forces – living or inanimate. You and I are ‘being’ wholes as individuals and yet also parts of family and social groups. As individuals ‘wholes’ we are made of parts such as our muscular skeleton structure and digestive systems. We are as we are because the parts collaborate to form the whole – in other words we show ‘emergent’ characteristics [15]. We see the NHS as an ecology of interdependent relations and interactions the behaviour and characteristics of which emerge from interactions between systemic processes – just as a whole jigsaw picture emerges from the interlocking pieces of a jigsaw
The successful delivery of a systemic process derives from the success of sets of processes in the adjacent layers. An important part of the identification of lower sub-system processes is that their successes are jointly necessary and sufficient for the process above – there is an explicit logical relationship connecting defined success, in all of its manifestations, at every level. It is also important to note that the layers are not hierarchical power structures. Rather they are levels of abstraction from setting policy down to detailed implementation. The attributes of each systemic process can be grouped under the headings of why, how, who, what, where and when. At each level the attributes can be identified (by multiple players) in a common format. These can then be implemented on a secure intranet to be accessed by those given authority to do so. Every process should have one ‘process owner’ responsible for leading the players involved in that process to detect and monitor progress, to identify potential unintended consequences and agree the required actions to steer the process to success. Success is defined as meeting purpose/aims/objectives and avoiding failure.
Practically we find it helpful to name a systemic process using the present participle or ‘ing’ form. For example, ‘Doing something’ – ‘Testing a blood sample’ or ‘Diagnosing a condition’. During the ‘piecing together’ or the ‘building of clusters’ systemic processes, changes and improvements will suggest themselves. For example, points of strategic dissonance may become apparent. This happens when an organisation hangs on to the old ways of doing things for too long because of a disconnect between actions and intent or purpose at any given level. For more on the details of this approach see [16, 17]
A Possible Strategy
In [4] we suggest that the key to driving change should be ‘influencing from the bottom up’. Top-down centralisation has proven ineffective [1]. Ham [18] writes ‘The overcentralised management of the pandemic was undoubtedly a factor in the failure to learn more effectively. Boris Johnson, the UK prime minister, and a small number of Cabinet members were visible in their leadership and appeared reluctant to draw on the expertise and intelligence of the devolved administrations, regional, and local government leaders. Opportunities for learning were lost, contributing to the mistakes that were made’. Policy decisions for change have to make sense to those ‘on the front line’ if they are to respond positively. That response is also conditional on the need for change to evolve up and down through the entire system. Given that policy makers and staff need to see how their decisions spread or percolate through the organisation we now propose that rather than describing the change process as ‘bottom-up’ we should regard it as being ‘inside-out’. By that we mean that change should be initiated at all levels of the system. The first stage of that change process is to identify the systemic processes at that level. Then by discussing the overlaps and interactions with ‘neighbouring’ systemic processes the people involved (led by the process owners) can adjust or adapt the systemic processes to fit. It is as if we are reshaping our jigsaw pieces so that they fit and interlock. These kinds of adapting change processes would not be ‘one-off’ and static. Rather they are dynamic systemic learningprocesses and an integral part of an ongoing improvement model. Organisational adaptability through feedback and learning is a key to success as successful change is shared and spreads out from many different points across the clusters to the whole organisation.
A strategy such as this will require high level policy makers and those allocating resources to also adapt and integrate. That can be difficult for political leaders who may be criticised by media and public alike for changing their policies. There are two solutions to this dilemma. One is to declare that running the NHS is no longer a political matter. The other is to take the opportunity given to us by the pandemic to initiate a different approach to openness to change when faced with a future full of uncertainty – with many unknown unknowns. This would require considerable political skill to persuade everyone in an accountable democratic society that certainty is simply no longer available in complex systems. Changing one’s mind is currently seen as a weakness and not, as it should be, a strength when fully justified by dependable evidence. Leaders will need to learn and adapt to facilitate the changes that will incentivise all those affected by their decisions to work differently. The strategy has also to apply to the totality of health and social care services of the organisations in and related to NHS England, including local authority social care and private companies.
In summary we suggest that the strategy to implement the laudable aims set out in the WP [1] should be to understand and motivate – not by imposing top-down targets but by ‘inside-out’ growing of clusters of understanding with commensurate motivation to ‘join up processes at multiple points and levels whether at the top, middle or on the front line.
Three Examples
We noted in [4] that the organisations reporting to the DHSC seem to be contributing to seven high level systemic processes. They are Commissioning Care, Providing Care, Supplying, Regulating, Advising, Educating and Researching. They will form our third example – see below. First, we present two lower level examples with a little detail (but still incomplete for space reasons) for illustration.
The method (a how question/attribute) we use to identify systemic processes begins with setting down, as a Mind Map [13] what people actually do. Figure 1a represents the systemic process of a GP ‘Consulting with a Patient’. Necessarily, as we have said, the diagram is incomplete. However, the main sub-processes shown are ‘Reviewing the patient record’, ‘Putting patient at ease’, ‘Diagnosing’ and ‘Managing further care’. The test for deciding on the nature of the sub-processes is to ask the question: ‘Would the successes of the sub-processes be jointly necessary and sufficient for the success of the process? Of course, each of these sub-processes has sub-sub-processes as shown. However, the sub -processes are self-similar in structure – they are each wholes and parts at the same time – which is why some people call them holons [16, 17]. A holon sub-process of ‘Diagnosing’ is ‘Requesting tests’ and a holon sub-process of that in turn is ‘Testing blood’ as highlighted in yellow. Each systemic process holon has a set of attributes gathered under the headings of why, how, who, what, where and when. In Figure 1a these are given in an abbreviated form. In a fully implemented Mind Map the attribute descriptions could be fuller and hold hypertext links to documents held on an intranet. For example, the (who) patient attribute could link to a Share Care Record or similar patient file. The {who) GP attribute could link to a GP Practice website of that GP. A link from the why attribute could link to present or previous symptoms. The Figure cannot show all attributes for all processes even as abbreviated. A further example shown in the diagram is that of ‘Prescribing’ with possible attributes also as shown. Figure 1b is a continuation of Figure 1a for the systemic process of
‘Testing Blood’. Subprocesses of ‘Making an appointment’, ‘Checking in’ etc. are shown again with abbreviated attributes. Of course, these processes are familiar and normally
well managed by GPs which is why we have given them as illustrative examples that relate to something familar.
Figure 2a is less familiar and more challenging. It shows an ongoing adjustment of systemic processes in the integrated Alliance Network of the fourth author. The process is ‘Enabling a Single Point of Access’ for mental health patients. Currently there are multiple points of access and these need to be integrated.
The processes highlighted in yellow of ‘Improving web access’ and Redesigning forms’ and Enhancing Teams are shown in Figure 2b. Clearly there are more processes and attributes to identify – for example ‘Consulting all involved’ and Checking fitness for purpose. Again a full description is not possible in this paper and work is ongoing.
A third example shown in Figure 3a is even more challenging. It is the top-level process of ‘Delivering Health and Social Care England’ and has the 7 sub-processes identified at the head of this section and in [4]. Sub-processes included are ‘Determining policy, ‘Allocating Resources’ and Integrating’ (highlighted in yellow). These are continued in Figure 3b together with ‘Regulating’, and ‘Advising’. Again, in each case we identify the attributes shown in abbreviated form for only some of the processes.
Clearly it is impossible here to capture the full richness of the processes and their attributes. That task can be made viable through adequate software operated by multiple players who ‘own’ each individual systemic process on multiple servers connected by an intranet. In the first instance only a simple mind Mapping tool is required but a full implementation will require adequate software with built in permissions and safeguards.
Improving Outcomes
The approach described could:
provide an overview of the whole organisational structure that
everyone can understand and appreciate which can be traced right down from the top level policy making down to the detailed ‘caring for patient’ processes;
allow people to identify overlaps and interdependencies. For example, advisory organisations could possibly be streamlined to co-ordinate advice and avoid incongruity and inconsistency;
enable caring for the sick, caring for public health and the vulnerable be under one ‘umbrella’ to avoid inconsistencies of policy over the longer time scales than politicians are typically in post;
enable a common data structure for the why, how, who, what, where and when attributes of each systemic process – important to avoid different groups using different data structures that cannot easily be shared and for data exchange via an intranet, with appropriate permissions to sensitive data, and the monitoring of progress and interventions to steer processes towards success;
enable all those involved in delivering success for the NHS to identify how the necessary and sufficient conditions for the success of systemic processes at the ‘coal face’ feedback into success and deficiencies at higher policy levels;
:;permit us to clarify;
pathways of precise terms of delegation and accountability – in particular;
how decision makers at all layers of the system delegate responsibilities down through the layers of processes – for example from government to NHS England and others to workers at the ‘coal face’ and ultimately to the patients;
how decision makers at all layers of the system are accountable up through the layers – for example from hospital ward care to Trust Boards, CCGs, NHS England and to government, parliament and ultimately to the public;
remove, reduce or ameliorate inconsistencies between policy and practice;
improve adaptability of response to unintended consequences and future unknowns such as pandemics and potential impacts from climate change.
Conclusions
The structure of Health and Social Care Services UK reporting to Government seems unhelpfully complex and opaque. We suggest a rationalisation using a ‘systems thinking bottom-up’ approach would be more likely to succeed than yet another top-down reorganisation.
Rethinking the interactions between existing organisations around ‘systemic processes’ could arguably bring considerable benefits including cost savings, better co-ordination, less ‘admin’ stress on staff at the ‘coal face’ and provide more organisational adaptability in an uncertain future.
Ultimately ‘systemic processes’ could help everyone deliver better patient care because that is the impelling purpose of the NHS.
References
Integration and Innovation: working together to improve health and social care for all [working title]. The Department of Health and Social Care’s legislative proposals for a Health and Care Bill. (2021, accessed 24th May 2021) http://www.healthpolicyinsight.com/?q=node%2F1699
Stirrat, GM, Blockley, DI, Alexander K, Phillips S (2020 The Structure of Health and Social Care Services UK – A thought piece at http://myengineeringsystems.co.uk/blog/
Timmins, N. The World’s Biggest Quango: The first Five Years of NHS England, (2018) The King’s Fund & The Institute for Government, UK
Hudson, A. Simpler, Clearer, more Stable: Integrated accountability for integrated care, (2016) The Health Foundation, UK
WHAT: A system, discriminated from its surroundings, is a set of models of our reality created by people for reasons which give meaning to and determine the purpose of the system
WHY: We identify a system because we are curious and want to understand (science), or wish to modify the world around us to improve the human condition (engineering, medicine) or express our emotions (art, religion). Our purpose in identifying the system is our highest goal. That goal provides us with meaning and motivates us to put in effort to add value. Identifying purpose draws on our emotional intelligence to help us reflect on and understand WHY we think and act, what we value and how we can improve how we work together.
Axiom: A2 of appropriate layers
WHAT: Systems models are holons i.e. they are both parts and wholes and hence are layered according to levels of detail and abstraction.
WHY: Thinking of a system in layers helps us cope with size, scale and dimensionality. Models of holons at different levels can be different but still be inter- dependent.
AXIOM: A3 of complex interdependency
WHAT: Holons are connected to certain other holons with which they exchange messages.
WHY: In a complex world everything seems to be interconnected and hence inter- dependent. Outcomes are often unintended. We can simplify by focussing on local connections in a manner similar to the internet of connected computers.
WHAT: A4 of the ubiquity of change
WHAT: Systems models change at varying rates but none are permanent and invariable. Some changes may be unforeseen. Some changes may be small but some may be ‘revolutionary paradigm shifts’ involving new ways of thinking.
WHY: Most of us think of matter or substance as the permanent stuff of which something is composed and form as the way that stuff is put together. Interestingly eastern traditions emphasise flow and change as things come into being and cease to be. This view ties in with the spontaneous random fluctuations of energy in a quantum space.
AXIOM: A5 of evolutionary learning
WHAT: Complex systems often cannot be ‘solved’ rather they have to be managed to desirable outcomes.
WHY: Learning reduces uncertainty. Learning is too often seen as rote learning of facts and techniques and ‘how to do something’. Learning to learn or ‘learning power’ has much to offer in finding our way through uncertainty.
What: Reality is actual but only accessible through human cognition
Why: We need to make explicit the notion that models are a representation of reality not the reality itself.
Corollary: C2 regarding worldviews
What: Systems models are created through the ‘spectacles’ of a set of worldviews.
Why: If models are a representation of our reality and not the reality itself we can think of the models as filters or spectacles through which we must look to see our reality.
Corollary: C3 regarding understanding
What: We can only control effectively what we understand.
Why: Perhaps this is self-evident but each of us understands in a different way. That is why we need to collaborate in teams to share understanding in different ways.
Corollary: C4 regarding embedment
What: Physical natural or artificial systems are ‘hard’ systems. Both are embedded in ‘soft’ people and social systems. Hard systems are objective whereas soft systems are subjective and intersubjective.
Why: This aspect of rigour sounds unduly ‘academic’ esoteric and remote from practice. However it underpins our understanding of uncertainty and the way we learn our way through it and so is important.
Corollary: C5 regarding functions
What: The purpose of a hard system is a function. The function of an artificial system is decided by us – it is man-made. A model of a natural system helps us understand the behaviour of a part of a reality. As a consequence we may ascribe a function to it.
Why: The function of man-made artefacts is a familiar concept to most of us. However the function of a natural system can be a source of confusion if we do not explicitly recognise that that function is ascribed by us through our models.
Corollary: C6 regarding fitness for purpose.
What: Hard systems are not universally true i.e. true in all contexts and circumstances. Rather they are dependably fit for purpose to a degree in a context. Dependability corresponds to our common-sense notion of truth or fact. Statements deduced from dependable models correspond to reality in a particular context or situation.
Why: Models, by their very nature are partial representations of our reality. Consequently they are incomplete and are only dependable in the context to which they are relevant.
Corollary: C7 regarding duty of care
What: The dependability of a systems model requires those people involved to exercise a proper duty of care, to test the model to an appropriately dependable level based on evidence, to demonstrate sufficient competence and integrity and to be transparent about their values.
Why: Dependability has to be judged based on the testing of a model. The tests have to be as searching and rigorous as appropriate for the problem. Practical rigour requires diligence and duty of care that leaves no stone unturned with no sloppy or slip-shod thinking.
Corollary: C8 regarding subsidiarity
What: The Principle of Subsidiarity (as set out in the Treaty of Lisbon 2007 [Eur-Lex 2016] is that systems models should be created at the lowest practical level consistent with delivering their purpose.
Why: The idea here is that decisions should be as local as possible because that is where the problems are best understood.
Corollary: C9 regarding emergence
What: Holons have emergent properties. These are attributes that apply at only one or more layers as a result of interactions between holons at lower levels that do not exhibit these attributes.
Why: Emergent properties arise or come forth from inter- dependencies at more detailed layers. They are more common than many people realise. For example the pressure of a gas is the result of the buzzing around of gas molecules at a lower level of description. The human ability to walk and talk emerges from the co-operation our many subsystems.
Corollary: C10 regarding connectivity
What: Connections create relationships and patterns of relationships.
Why: In Chinese thought all things are interconnected. The internet is a web of interconnected computers. The brain is a network of highly interconnected neurones. Our infrastructure is an interconnected network of facilities.
Corollary: C11 regarding stakeholder interests
What: There is an increased chance of success if stakeholder interests are aligned.
Why: Common sense tells us that we are more likely to be successful if we ‘pull together’ as oarsmen do in a boat race. We are more likely to pull together if we have a common purpose.
Corollary: C12 regarding processes
What: Systems models are processes.
Why: If we accept that change is ubiquitous then everything is a process. Why is this helpful? Because it shifts our focus and leads to a new understanding of change. It provides us with a means of integrating many ideas and enables us to create simplicity in complexity. Unsurprisingly perhaps many people find it hard to think of a table as a process since they cannot reject the idea that it is a thing composed of ‘stuff’ – such as wood. It may help to think about the life cycle of the table from raw material, through design and making to usage, maintenance and disposal to see the table is constantly being and becoming. Everything exists in the process of time.
Corollary: C13 regarding feedback
What: Processes may be loopy involving feedback and feedforward.
Why: Most engineers are familiar with the ideas of feedback and feedforward in hard systems. They apply equally in soft systems where they are often called loops of influence.
Corollary: C14 regarding leadership
What: Managing a process to a desirable outcome requires appropriate leadership and collaborative learning.
Why: Traditional learning is something we do to acquire knowledge that may be useful to us in some way. We tend to think via a prescribed framework which promotes a strong distinction between the academic and the vocational which devalues practical wisdom. To change, people need vision. Leadership is about engaging with that vision then building and coaching teams to achieve it – and it applies at all layers.
Corollary: C15 regarding outcomes
What: Unexpected and unintended changes may result in future consequences that may be opportunities to create benefit or hazards that threaten damage.
Why: We must protect ourselves from the harmful effects of unintended consequences that is why we need to be alert to the possibility of ‘incubating failure’. Just as importantly we must take advantage of possible benefits from unintended consequences – they lead to new opportunities and genuine innovation.
Corollary: C16 regarding the six ‘honest serving men’
What: Attributes of processes can be classified into the categories of why, how, who, what, where and when. ‘Why’ expresses the purpose which drives the ‘how’ of the methods, transformations and procedures of change in the descriptors and measures of people (who), performance indicators and systems variables including impedance (what), contextual influences (where) and measures of time (when). One way of expressing this is ‘why = how (who, what, where, when)’.
Why: Rudyard Kipling’s six good men are generic. They provide the means to capture, model, control and improve processes in systems.
Corollary: C17 regarding ‘trade-offs’
What: Trade-off decisions may be required when two or more output variables are negatively related. For example the trade-off between lower NOx and lower CO2 pollution in exhaust gas recirculation of a diesel engine. A balance of disadvantages may have to be struck. For complex systems, the balance between the multiplicities of variables becomes even more difficult.
Why: Axiom 5 states that complex systems often cannot be ‘solved’ rather they have to be managed to desirable outcomes. One of the means of managing trade-offs is through evolutionary learning recognising that many trade-offs are non-linear and step changes may be created by innovation.